The Synergy Model An insight into Synergy, its success in the treatment of the symptoms associated with
Post Traumatic Stress Disorder/Response (PTSD/R) using Spectrum Therapy as the emotional change intervention
Executive Summary
The SynergyTM programme is a coaching based therapeutic personal development protocol, designed by Michael Stott. It uses a non-medical, client- centred approach, combining talking therapy and coaching tools in the form of Spectrum TherapyTM and Hypnosis. SynergyTM has had significant success with a growing population of clients, many who have not achieved results with other established models. It was designed and trialled in 2006 and has since undergone continual development to adapt it to a range of specialised populations. Client Base Synergy TM has been at the forefront of therapeutic coaching and personal development programmes since its initial introduction being as it is the only programme specifically designed for the purpose of working with the sufferers of Post Traumatic Stress Disorder (PTSD) and is the protocol which is validated according to evidence based results. It has been successfully used with a broad spectrum of clients including current members of the uniformed services, veterans and individuals suffering from addiction, who have been in the mental health system presenting the symptoms associated with and other stress related problems. Number of Participants and Analysis. Over 2000 individuals have participated in treatment and personal development programmes linked with the programmes ongoing development. As SynergyTM has matured anecdotal evidence from case studies have proved to be overwhelmingly conclusive, details of which are included in this paper underlining the need for academically rigorous statistical analysis. Detailed data has been collected for the 84 participants who have completed the latest version of the programme and additional research is now being carried out by Wolverhampton University, in conjunction with a statutory drugs and alcohol rehabilitation service and a national charity supporting the suffers of PTSD, this is due to be published in 2011. Measurement SynergyTM has been measured with a variety of instruments that are recognised by both the World Health Organisation and the UK Military research establishments. Wolverhampton University are using different measurement instruments that are more relevant to their specific requirements of their research.
Permanence of Change Measurements were taken before and after the four-day programme, with follow up checks 6 and 12 months later to establish the permanence of change. A number of illustrative case studies have been included in this paper to demonstrate the impact of the SynergyTM Programme with lasting behavioural change demonstrated and recorded up to 5 years post SynergyTM programme attendance. Current Options Individuals suffering from PTSD or Complex PTSD (often described as a more chronic and more pervasive negative condition) are currently offered a choice between Cognitive Behavioural Therapy (CBT), Eye Movement De-sensitisation Re- processing (EMDR), Counselling and Drugs, or a combination of these. This is true both within the military medical services and the National Health Service (NHS). Inadequacy of Options Many of those who have sought out the Synergy TMprogramme report that the approaches detailed above have proved ineffective for them and often left reporting they believe there symptoms have intensified post treatment with the current options. In many cases those whom have undergone repeated treatments are often left believing that they are incurable and will suffer the ill effects of PTSD for life. Synergy Support Network The Synergy TMprogramme is designed to resolve problems, ideally before they become embedded and complex in nature. It offers continued support to all participants through a network of supporters with similar experiences and shared adversities. The network includes specially trained supporters for those who experience continuing difficulties, providing a service that to date has been unavailable to veterans suffering from complex PTSD, and their families. Independent Analysis In 2010, Stott, in co-operation with two PTSD charities, commissioned independent statistical analysis of the data captured during the SynergyTM programmes, which conclusively showed that the SynergyTM programme can produce highly significant benefits to PTSD sufferers and their families. The detailed findings of this report are at Annex A. All participants in the SynergyTM Programme complete a number of instruments1, recognised by both the World Health Organisation and the UK Military, to measure their current reaction to the symptoms they are experiencing. These instruments are subject to Analysis Of Variance (ANOVA) to establish statistical
1
Depression Anxiety and Stress Scale (DASS), PCL (Military) and General Health Questionnaire (GHQ)
significance and formed the basis of the statistical analysis of the SynergyTM Programme. Continuing Analysis Analysis continues and further data is being gathered. A 5-year case study review has been conducted of the original participants from 2006, which shows long- term behavioural change. A rolling review has been put in place to build the evidence for the programme’s long term efficacy. Adaptability A key strength of SynergyTM is that the core elements can be tailored to suit specific needs. These include PTSD in different populations, drug and alcohol abuse and disenfranchised prisoners. The elements to the programme can be applied remedially and generatively which makes it adaptable and unique. The Future Stott and his team intend to seek acceptance of SynergyTM as a recognised model to be used within the context of mental health and wellbeing. A SynergyTM Practitioner development plan is in the process of being implemented to ensure the replicability of the SynergyTM Programme in the future. Practice Synergy TM is a product that can be licensed for use by trained practitioners, which takes on average approximately 2 years and includes mentorship, peer revue, and reflective practice. Successful candidates are awarded the title of SynergyTM Practitioner and are licensed to work directly with PTSD sufferers, with access to support from The Synergy Institute CIC. Governance Synergy TM is governed by The Association of Synergy Coaching CIC, an external body comprising experienced professionals from different backgrounds including education, medicine, mental health and alternative approaches. The Synergy Institute CIC was established to guide, educate and regulate its membership for the purpose of quality assurance and ethical adherence of its programmes, which are available to all practitioners of therapy and personal development. Conclusion SynergyTM has demonstrated it ability to make a real and significant difference in the lives of those individuals who have undergone a 4 day SynergyTM Programme as reported by those who have attended. The statistical analysis detailed at Annex A shows that 97% of scores for Depression, 91% for Anxiety and 100% for Stress were in the normal category post-treatment with no score higher than Moderate.
Annex A Report on the study of the effect of Synergy on persons suffering from symptoms associated with Post Traumatic Stress Disorder/Response (PTSD/R) Author: Christine Wood
BSc, FRSS, PgDip (applied statistics) Wood Independent Statistical Services
Index Background
Introduction
Methods
Results
Conclusion
Summary
Appendix Statistical Calculations References
Background
Post traumatic stress disorder was first recognised as a disorder in the third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III)1 and the International Classification of Diseases tenth edition (ICD-10)2. The past 25 years has witnessed a dramatic increase in the clinical and scientific information concerning the diagnosis and assessment of post traumatic stress disorder (PTSD) (DSM-III)1. Several comprehensive, multi-scale, self-report instruments are available to clinicians to address dimensions such as re-experience, avoidance, emotional numbing and hyperarousal, these have been widely acknowledged and regularly reported symptoms of those who have been diagnosed with PTSD. There are many instruments that can be used to measure the effects and symptoms of PTSD on the sufferer and a number also require further input by an appropriate clinician. Therefore the capturing of reliable data was governed not by the number of patients but by the availability and objectivity of an appropriate clinician. The role of the appropriate clinician sits as the key factor of the critical path for reliable data collection in the PTSD environment; which potentially explains why there is a limited volume of reliable data available in relation to PTSD compared to the number of diagnosed suffers. Introduction to the Study The collection of reliable and robust data around any therapeutic intervention is essential to ensure that is was collected in a timely and appropriate manner; which could facilitate the entire population of all those engaging in the therapeutic process. Therefore the study required a mechanism of collecting data that need not to directly depend on an appropriate clinician. A suitable instrument which was clinically recognised, would allow for the collection of robust subjective data that allowed self-completion, was easy to use, reliable and able to measure any change in symptomology was chosen. The design methodology for this study needs to support the collection of data to be able to facilitate an appropriate measure of the impact of the therapeutic process on the individual PTSD sufferer. The design could be summarised as follows:
A non-medical alternative approach as outlined by the National Institute of Clinical Excellence.
Utilise group interaction and psycho-education around performance and analysing perception of experience.
Individual consultations using the key elements on a number of talking therapies Neuro Linguistic Programming (NLP), Spectrum TherapyTM and Hypnotherapy. These have been combined in a bespoke therapeutic programme called SynergyTM.
The utilisation of the outdoors for creating change self-expression..
Telephone and e-coaching programme pre and post course.
Suitably qualified practitioners in accordance with the recognised awarding bodies of the above disciplines and Synergy. The studies methodology was piloted in 2006 and this confirmed to appropriateness of
the study design. The Study Population The research population was anyone suffering from the symptoms of PTSD. In order to proceed we needed to take a sample of this population to participate in a study and engage in the SynergyTM therapeutic process. The study sample is based on the following criteria: All diagnosed as suffering from PTSD via a General Practitioner by a Psychiatrist.
All have undergone therapies as recognised by NICE and have continued to be diagnosed as sufferers of PTSD by a General Practitioner or Psychiatrist.
All volunteered to attend. Clients are from both uniformed and civilian backgrounds who have been involved in operational environments associated with PTSD/R; they include Police, Fire Brigade, SAS Soldiers, Paratroopers, Royal Marine Commandos, Royal Navy, Royal Air Force and sufferers of domestic violence. Some of these presented extreme symptoms of PTSD which included; alcohol dependency, drugs abuse, self harming, violence to others and suicidal tendencies. Five clients were involved in the pilot study. The study has progressed and a further 70 clients have undergone treatment. It is their results which are included here. Process and procedures were refined following the pilot study, with a final choice of instruments for 6 and 12 month follow up. There are many instruments in circulation for detecting anxiety, stress, depression and other symptoms relating to PTSD/R, the following were considered
Impact of Event Scale (revised)3 this parallels the DSM-IV17 and is a reliable instrument but analysis was on a basic score with no validity or checks for gender or age
Trauma Symptom Inventory3 shown to be reliable with norms available for age, race and gender. Instrument copyrighted and not available for use.
Posttraumatic Stress Diagnostic Scale3 reliable but time taken to complete as long as 15 minutes, if items incomplete analysis invalid
Depression Anxiety Stress Scale (42)4 a valid and reliable self-completion instrument, quick and easy to complete norms available gender and age found to be negligible in assessment process. Instrument is in the public domain along with norms.
Beck Depression Inventory (BDI) 5 used extensively but only identifies depressive state.
Beck Anxiety Inventory (BAI) 6 designed to discriminate anxiety from depression. Well validated Other instruments were investigated but have not been included. The instruments to be used pre treatment are the PCL-C13, the DASS (42) and the GHQ1214 with the DASS used post treatment and the PCL-C and DASS used on follow up. All of these instruments have been shown to be reliable and have both construct and content validity. The reliability and validity of the PCL-C have been widely established. The Posttraumatic Stress Disorder Checklist-Civilian Version (PCL-C) is a 17-item self-report measure of PTSD symptoms for adults as based on DSM-IV criteria, respondents indicate on a 5-point Likert scale ranging from 1 (not at all) to 5 (extremely) the applicability of statements for the past month. A sum score of 50 or more merits a PTSD diagnosis. Internal consistency is high and validity is also supported by high correlations with other validated measures of PTSD13 These instruments are fast and easy to complete.
The DASS can detect change in a 5-7 day measure period.
The PCL-C has been shown to be an effective diagnostic tool
Each client completed the PCL-C DASS and GHQ12 on first arrival at the centre.
The DASS is a simple scoring system with a rating of 0 to 3 for each question.
The scores are totalled and give a score for depression, anxiety and stress they are then combined to form a total score.
DASS Scoring Norms
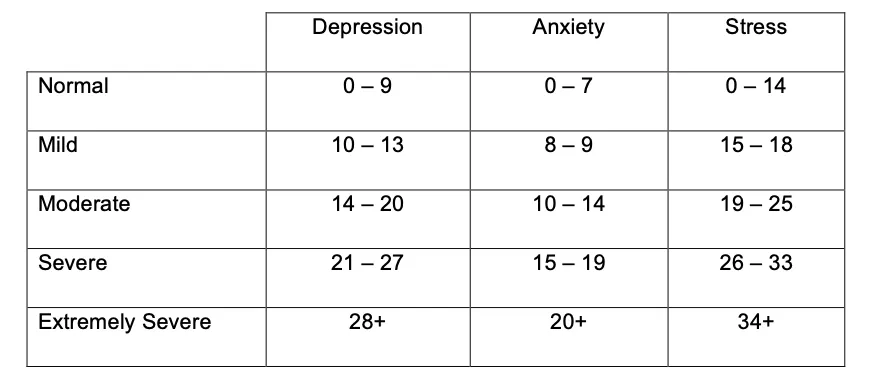
There are 42 items with 14 items per scale, maximum score of 126 minimum score of 0. Raw scores have also been converted to z scores using the norms produced by Lovibond & Lovibond (1995)10 and Crawford & Henry7. Norms produced by Lovibond & Lovibond have been used extensively but were developed on a student population whilst those developed by Crawford & Henry on a more generic population, both are included for completeness. There are two possible methods for scoring the PCL-C
a) Sum up the score for each question to give a final score. A score of 50 or more being symptomatic of the presence of PTSD/R b) questions 1- 5 B (Intrusion) questions 6-12 C (Avoidance/Numbing)
questions 13-17 D (Hyper Arousal)
A score of 1B, 3C and 2D being symptomatic of PTSD/R. Norms used by the Armed Forces were type a) and have been used in this analysis the instrument has a maximum score of 85 and minimum score of 17.
Type b) category counts are associated with the DSM IV.
GHQ12
a) This has 4 scales with responses on the first two scales coded 0 and the last two coded 1. This method gives a maximum score of 12. Using just binary variables (0/1) is sufficient for identification of PTSD/R (score greater than 4 being indicative). b) Scoring each question 1 to 4 and totalling all scores pre and post treatment. Maximum score of 48 minimum score of 12
The total scores (b) have been used in the analysis with the scores in a) given for completeness and used as an indicator where PCL-C score was less than 50 All forms were returned for statistical analysis which was performed using Minitab 15 and Excel. The individual scores for each item were subject to analysis with each client having 2 scores one before treatment and another post treatment, the object being to see if there was any difference in each of the areas measured by the instruments after treatment. Methods used include paired t-tests, normal probability plots and examination of means and z scores pre and post treatment compared to published norms. Assumptions made:
Clients were not specifically chosen but responded to open invitation followed by GP authorisation
Clients suffered from a traumatic event
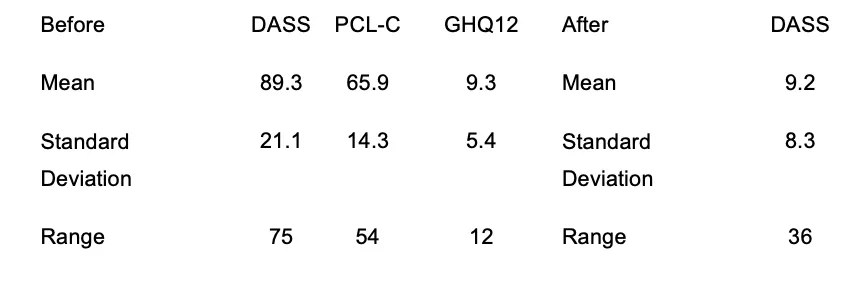
Diagnosis of PTSD/R made by a clinician Results Mean scores for before and after for each category are shown below along with respective standard deviations. (Standard deviation being a measure of variability from the mean) Of the 70 clients 2 were excluded as not satisfying any of the instrument criteria for diagnosis of PTSD and had unrealistic DASS scores, information on these clients was obtained from the practitioner as follows “from work with this particular population it is our opinion that guided self report is sometimes flawed, which can be attributable to denial or cognitive dissonance and the subject not wishing to be a burden or not wanting to be seen to over exaggerate what they were really experiencing. Even when clinical diagnosis is established participants display these limitations when self- reporting. Self-reporting can also be influenced post programme, as change is experienced quickly and the participant can still be dissonant to the new conscious
acknowledgement of change. Participants often realise change when they return to their home environments reducing dissonance gradually and establishing behavioural change. “ Average age was 39.3 years with 56 males and 12 females range was 39 (63 – 24). Clients who had a score less than 50 on the PCL-C were checked on other criteria using alternate PCL-C method and/or GHQ binary score


Clients’ score pre-treatment were higher than the scores in the ‘Normal’ population

The mean values are in the ‘Extremely Severe’ scales pre treatment
66% of scores for Depression, 72% for Anxiety and 51% for Stress were in the Extremely Severe category pre-treatment

97% of scores for Depression, 91% for Anxiety and 100% for Stress were in the normal category post-treatment with no score higher than Moderate.

The scores in the above bar chart were calculated from the ‘Norms’ in Table 2

The diagram shows the change post-treatment with clients’ scores in the ‘Normal’ range (below 0.5)
The z-score for symptoms can then be grouped into:
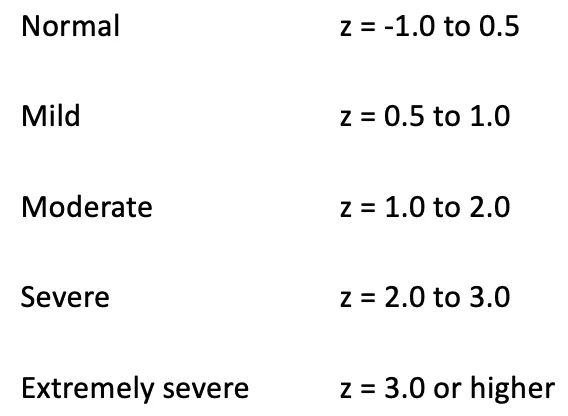

The higher the z score the more severe the symptoms, a score at or below 0 signifies emotions within normal range.

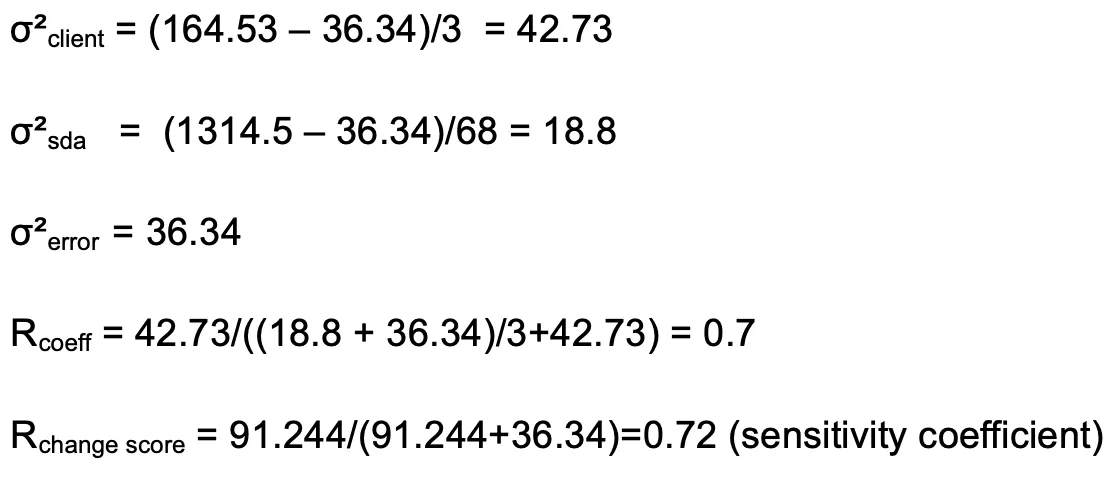
The analysis of measurement instruments along with change scores is the subject of much debate9,10. In measuring change it is important to ensure the reliability of the instrument with the data to be analysed. The method used is as proscribed in Health Measurement Scales (Strainer D, Norman G)8
The reliability coefficient was 0.7 (variability between clients) (1 being excellent 0 being none) change scores should only be used if this value is >= 0.5 , the sensitivity of the instrument to detect change was 0.72 this expresses the proportion of the variance in the change score due to ‘true’ change. As change falls within satisfactory limits analysis can be performed on the change scores (post-test minus pre-test scores)
Having determined the reliability further tests are required as to the normality of the scores to be analysed. If the data is not approximately normally distributed it may be necessary to use different non-parametric techniques (these are not as powerful). Normal probability plots to determine if the difference (this value is the pre-test – post-test) is normally distributed for DASS is shown below.





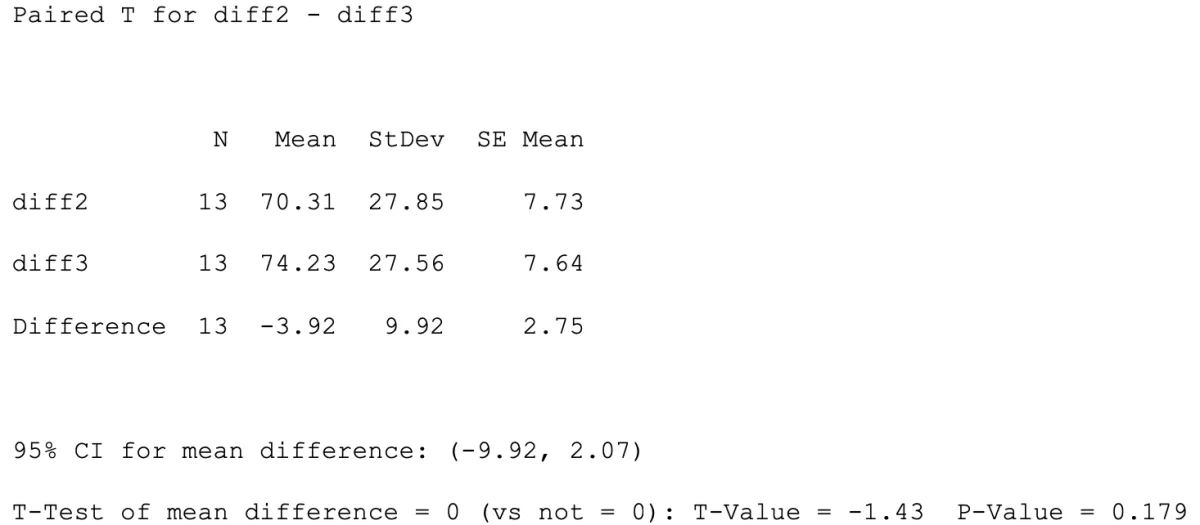
The plots are for total difference score Fig2, Depression Fig3, Anxiety Fig2 and Stress Fig1also included are Normal plots for 6 and 12 month Follow Up. A p-value less than 0.05 would have led to consideration of the use of other techniques, the normal distribution is robust on some assumptions but the above cases test conditions are satisfied as all the plots have values greater then 0.05. A paired t-test was performed on the difference between the post-test and pre-test scores with the following hypothesis: Null hypothesis: There is no change in the scores after treatment (mean = 0) Alternative Hypothesis: that the change score is less than 0 showing an improvement by a reduction in scores (giving a negative difference). 1 sided test at 5% (p = 0.05) Reject the Null Hypothesis accept the Alternative Hypothesis results from the test showed there to be a highly significant difference (p=0.000) in scores. A paired t-test was performed on the difference between the first difference scores and the 6 month Follow Up difference scores (n=13) with the following hypothesis Null hypothesis: There is no change in the scores after initial treatment and 6 Month Follow Up (mean = 0 no change indicates treatment still effective after 6 months ) Alternative Hypothesis: There is a difference between initial treatment and 6 Month Follow Up scores Accept the Null Hypothesis there is no significant difference between the pre /post test scores after initial treatment and the pre/post test scores at 6 Month Follow Up( P-Value = 0.179)
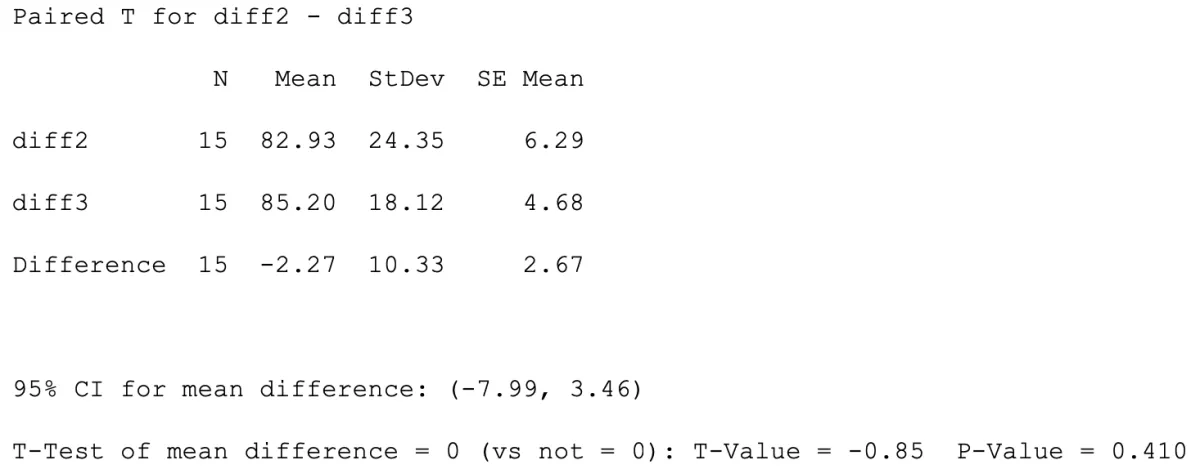
A paired t-test was performed on the difference between the first difference scores and the 12 month Follow Up difference scores (n=15) with the following hypothesis Null hypothesis: There is no change in the scores after initial treatment and 12 Month Follow Up (mean = 0 no change indicates treatment still effective after 12 months ) Alternative Hypothesis: There is a difference between initial treatment and 12 Month Follow Up scores Accept the Null Hypothesis there is no significant difference between the pre /post test scores after initial treatment and the pre/post test scores at 12 Month Follow Up ( P-Value = 0.410) Conclusions A basic analysis has found that following intervention scores decreased significantly, 97% of scores for Depression, 91% for Anxiety and 100% for Stress were now in the Normal category post-treatment with no score higher than Moderate, a significant improvement for all candidates. Follow up instruments at 6 and 12 months show that candidates remain stable, and that there is a significant improvement in the quality of life of all candidates. Instruments will continue to be sent to clients 6 month and 12 month post treatment and results updated accordingly. Synergy has shown significant benefits in a short timescale for sufferers of PTSD/R, which has been maintained by candidates during their first 12 months post treatment.
Appendix Minitab Analysis Paired T-Test and CI: time1, time2 (DASS scores; time1=pre treatment time2=post treatment)
Paired T for time2 - time1
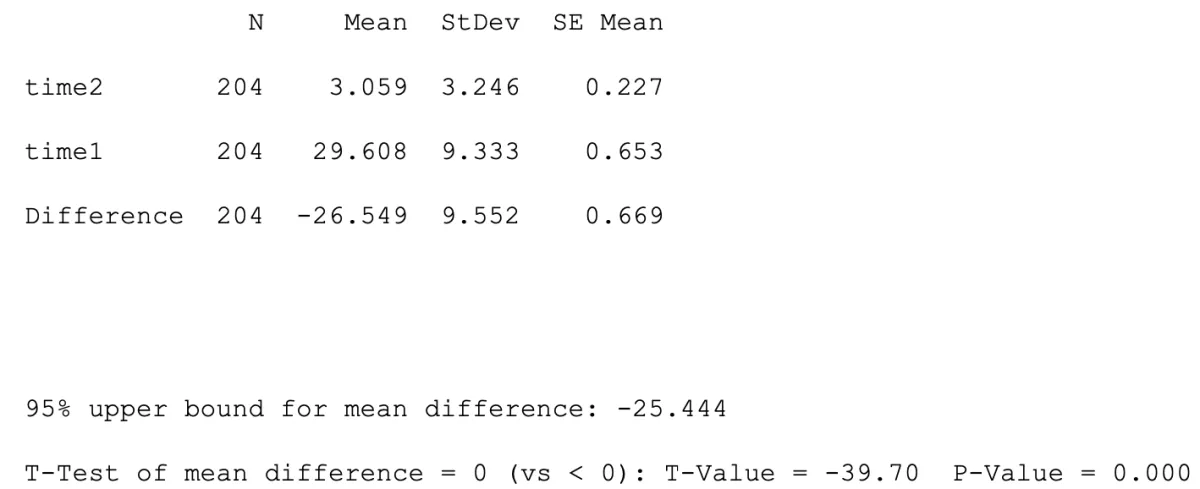
One sided test used as looking for improvement in condition and not a change in either direction.
Paired T-Test and CI: diff2, diff3
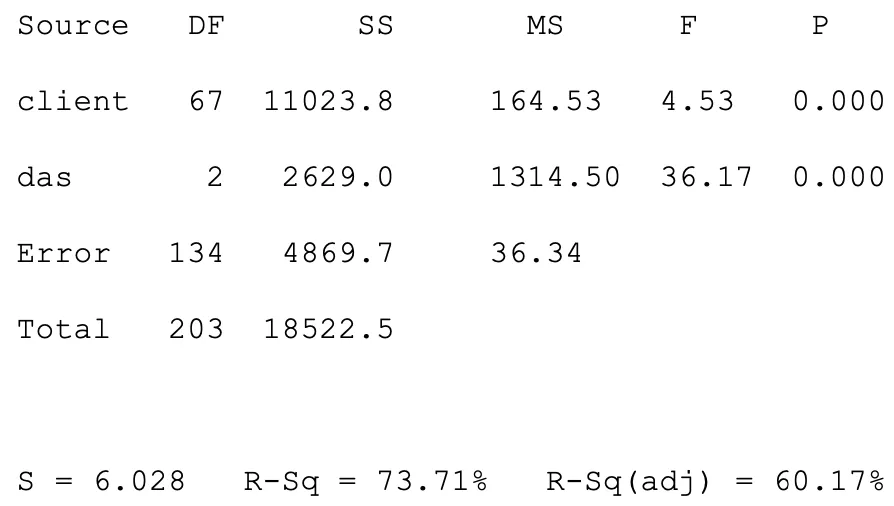
Two-way ANOVA: difference versus client, das
Reliability calculations
Descriptive Statistics: difference